Safe Supply as Treatment
Covid-19 has made the opioid crisis worse. One reason is that Covid has led to increases in stress, financial hardship, and isolation, so people are seeking out drugs at a higher rate than before. Supply lines have also been disrupted. This has forced people who use drugs to get their supply from unfamiliar sources, which increases risk.
These patterns have given extra incentive for those arguing for policy change, and in some places, policymakers are willing to try new strategies in recognition that current drug policy doesn’t work. The ‘war on drugs’ approach of criminalizing the possession of even small amounts of drugs has only exacerbated their negative effects. A different approach, which decriminalizes possession, is getting more support. Oregon recently voted to decriminalize the possession of small amounts of illicit drugs. In Canada, the Canadian Association of Chiefs of Police released a report in July 2020 recommending drug decriminalization.
Another approach is safe supply. A substantial number of deaths due to opioid use are unintentional and are at least partly due to the drug’s unknown strength and composition. In British Columbia, about 80 percent of drug-related deaths in 2020 have involved illicit fentanyl. Therefore, providing people who use drugs with safe supply would address a primary source of harm.
Safe supply also helps address other effects of drug use, including the crimes people commit to buy drugs. It’s one option in the ‘harm reduction’ approach, which seeks to reduce harms associated with activities instead of treatment that aims at eventual abstinence. Other examples include needle exchanges, which prevent transmission of diseases such as HIV. (And save money: for every dollar invested in such programs, taxpayers save around six dollars for decreased HIV treatment costs alone.)
Although safe supply programs are understudied, there is evidence that they’re effective. One study, called NAOMI, found that providing heroin instead of methadone led to higher treatment retention, much lower spending on drugs by participants, and significant improvements in “medical and psychiatric status, employment satisfaction, and family and social relations.” These and similar findings in other studies have attracted government attention. In October 2020, the Government of Canada announced funding for a safe supply project in Ottawa.
There’s enough evidence to make safe supply worth trying. Along with other changes to policy, it will prevent the worst effects of the opioid crisis.
Is Safe Supply Treatment?
An important question about safe supply is how it should fit into broader drug policy. There’s a concern that safe supply is a dead-end approach, since it doesn’t aim at the root causes of drug use. Further, it’s giving people the very drugs that are the problem. In response to objections of this sort, safe supply advocates argue that providing drugs constitutes treatment. Dr. Keith Ahamad, an addiction in physician in Vancouver, puts it this way:
I’m not feeding their addiction, I’m treating their addiction. By prescribing heroin to a heroin addict, if I’m able to eliminate crime, if we’re able to eliminate human suffering, if we’re able to eliminate all the expensive health care costs associated with illicit heroin use, then we’ve achieved our objective of treating their addiction (1).
Another way of framing Ahamad’s argument is that it isn’t the addiction per se that’s causing the bulk of issues for people who use drugs. Instead, it’s the myriad effects of current drug policy that cause problems. If people can use heroin without having to commit crimes to get it or risk the serious health outcomes of taking street drugs, then this is a big improvement.
In response, Dr. Jeremy Devine, a psychiatry resident in Ontario, argues that the ‘safe supply as treatment’ approach is indefensible:
Under the harm reduction paradigm, individuals are considered “treated” if they remain alive and are not actively committing crimes or using health care resources. This approach compromises the potential of the drug user, who is now viewed as a liability to be managed rather than an individual with potential gifts to offer (2).
Devine is essentially voicing the dead-end worry. In his view, merely reducing the harms of drug use counts for little if the person is still using drugs, since continued reliance on drugs prevents flourishing. Treatment has to get to the root of the problem.
This disagreement between Ahamad and Devine just is the disagreement between the traditional, abstinence-directed approach of addiction treatment and the harm reduction approach.
The first step in assessing these views is considering if safe supply should count as treatment at all. Here we face an essentially definitional question: what does it mean to treat someone? It might be tempting to propose that treatment aims at curing the medical condition afflicting the individual, but more reflection reveals that this is too narrow. Lots of forms of treatment occur even though no cure is in sight.
Consider palliative care, which aims to ameliorate suffering to improve quality of life precisely when curative options either don’t exist or are not worth it. Or consider insulin therapy for diabetes. Presently, there’s no cure for diabetes, so people with diabetes take insulin to manage the negative effects of their condition. Since both palliative care and insulin are standardly considered forms of treatment, the definition of ‘treatment’ can’t turn on the intervention aiming at a cure.
A better definition is broader: Someone is receiving treatment if they are receiving care that aims to reduce the negative effects of a medical condition. This captures the two examples above, and others. One implication of this definition is that it says nothing about addressing the root cause of the medical issue. So, if I take acetaminophen after breaking my arm, I’m treating my broken arm by slightly reducing the pain I feel, even though I haven’t yet done anything to actually address the broken bone. But this implication isn’t really such a problem. Palliative care isn’t addressing the root cause—that’s what makes it palliative care—and the broken arm example just shows that there are better and worse forms of treatment. I’d be much better off seeking professional help.
Another point to note is that, while one must have a medical condition to be treated, the effects of the condition don’t need to be medical. Consider a roofer who develops carpal tunnel syndrome in his forearms, and suppose that this is only a problem since his job involves lifting heavy equipment. It doesn’t affect the rest of his life. In this case, the treatment he receives—surgery or physical therapy—is aimed at addressing his inability to work.
All of this leads to the conclusion that safe supply is a form of treatment. It’s given to people who use drugs for the purpose of ameliorating the negative effects of their addiction. Devine’s objection is really two-fold. He says “One can reasonably question where exactly the treatment lies in injectable opioid agonist treatment. Does this treatment empower patients?” (2). The answer to the first point is that the treatment lies in its ability to ameliorate negative effects of addiction, just as insulin ameliorates the negative effects of diabetes. Those who claim that safe supply isn’t treatment either misunderstand what treatment is by defining it too narrowly, or don’t see that safe supply can address the effects of drug use.
Is Safe Supply a Good Option?
Devine’s main concern about safe supply is that it falls short of ‘full’ treatment. He grants that it can address some negative effects of drug use, but argues that it “compromises the potential of the drug user” by not empowering them to take full control of their lives by quitting their drug use. For Devine, safe supply is like putting a diabetic on lifelong insulin if there were a cure for diabetes available. The insulin is better than nothing, but it isn’t the best option.
However, there are important ways this analogy doesn’t work. One is that there is a non-trivial number of drug users for whom standard therapy such as methadone is ineffective. They will likely return to using street drugs without safe supply. There’s also some number of drug users who never start treatment. Some find it too onerous, while others simply don’t want to give up drugs. Once again, safe supply could benefit them.
A few things need to be true for Devine’s argument to hold. One is that safe supply would have to become the predominant treatment option, so that people who are currently receiving treatment would switch to safe supply, thereby preventing them from getting treatment that aims at abstinence. This might be the case, but it isn’t necessarily so. Ahamad frames his use of safe supply as an option for those for whom other forms of treatment have been ineffective, whereas Devine writes as though safe supply is going to replace all other options. The reality will probably be somewhere in between.
For Devine’s argument to work, it must also be true that the overall costs of safe supply have to outweigh its benefits. (I mean this broadly, not just financially.) It’s also far from obvious that this will happen. He rhetorically asks if safe supply empowers patients, with his presumed answer being ‘no’. But this is debatable.
The Canadian Association of People who Use Drugs (CAPUD) argues in favour of safe supply in part because, it believes, safe supply increases autonomy. One of its images is of handcuffs coming off a person and the words “safe supply means freedom” in big letters (3). Freedom is pretty close to empowerment, and we should defer to the preferences of the very people these policies are trying to help. While CAPUD partly means freedom from prosecution, it also has in mind the freedom to use drugs if one wishes. The only options shouldn’t be street drugs or full treatment.
Back to the cost-benefit assessment. Devine’s view is that drug policy ought to aim at full empowerment through treatment, with the goal of abstinence. The safe supply view is that policy should aim at addressing the worst effects of the current drug crisis—especially overdose deaths—in concert with other strategies. CAPUD puts it this way: “Safe supply is a drug policy category that ought to fit alongside other ‘pillars’ of drug policy such as treatment, harm reduction, education, and prevention” (3).
The stark way of putting the tradeoff between the two views is that, if the assumptions about efficacy are correct, then following Devine’s plan will lead to more people off drugs but more deaths. In contrast, safe supply is willing to take the risk that some people won’t make it as far in treatment for the benefit that fewer will die and suffer the other negative effects of illicit drug use.
The problem is that the data are sparse. We don’t know what the tradeoff will be if safe supply becomes widely available. Still, we can make enough progress to consider whether safe supply trials of the sort Ottawa is trying are worthwhile. And we can do it using graphs.
Consider how you would fill in Figure 1, where the x-axis represents treatment progress and the y-axis is overall value (i.e., how good it is for the individual and the community for someone to make it through treatment). Let’s assume that there’s overall value in being completely off drugs: i.e., all else equal, it’s better to be not using drugs than using drugs. Without intending to beg the question, I’ve marked ‘safe supply’ and ‘abstinence’ on the x-axis so there are consistent markers.

Here’s the general shape of Devine’s view:
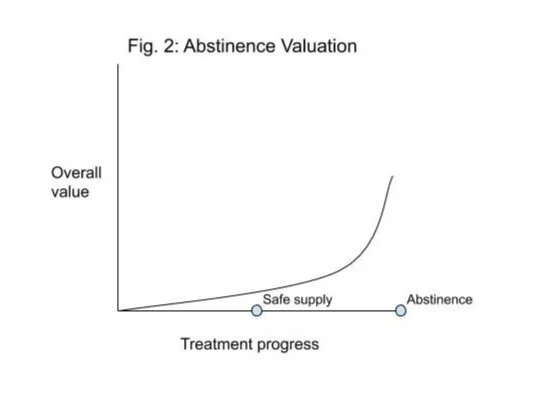
Here’s the safe supply shape:

The difference is that Devine thinks much of the value of treatment is from the person being ‘fully treated’ (i.e., no longer using drugs). This is why he’s against safe supply. In his view, it doesn’t empower individuals to a sufficient amount. In contrast, on the safe supply approach, there is comparatively more value in getting to the stable point of using safe supply, even though one is still using drugs.
Another way of putting this point is that, for safe supply advocates, there’s a bigger gain from nothing to safe supply than there is from safe supply to abstinence. Safe supply prioritizes getting people to the stable point of safe supply—which has a decreased risk of overdose, fewer negative health effects, and improvements in multiple lifestyle factors—and then offering other treatment for those who want it. Some will go on to treatment that aims at abstinence, which has some value. But those who don’t still benefit from safe supply.
The case for safe supply is that it’s better to address the worst effects of behaviour, even if that means the behaviour itself will persist. When we think about drug use, its worst effects aren’t due to the drug itself—though there are negative effects of using drugs—but the other consequences of current policy. The best reforms will increase access to other forms of treatment, but safe supply is worth including.